News & Publications
Determination of “Indeterminate” Thyroid Nodules
October 25, 2012
By Felix Martinez Jr, M.D.
A thyroid nodule is a discrete lesion within the thyroid gland. It may or may not be palpable. Palpable thyroid nodules are usually discovered on physical examination, but could be felt by the patient initially. Nonpalpable nodules often are incidentally discovered on CT and have been termed “incidentalomas”. Nonpalpable nodules have the same risk of malignancy as palpable nodules of the same size. Clinical guidelines suggest that only nodules larger than one cm be further evaluated, since they have a greater possibility of being malignant. Sometimes nodules smaller that one cm require evaluation because of suspicious ultrasound findings, associated lymphadenopathy, a history of head and neck irradiation or a family history of thyroid cancer.
Thyroid nodules are a common clinical problem, and differentiated (i.e., papillary and follicular) thyroid cancer is becoming increasingly prevalent. The American Thyroid Association (ATA) published revised guidelines for the management of these disorders in 2009. This is a comprehensive revision of the guidelines for the management of thyroid nodules, recommendations regarding initial evaluation, published clinical and ultrasound criteria for fine needle aspiration biopsy and guidelines for interpretation and reporting of !ne needle aspiration biopsy results, including algorithms for the management of benign thyroid nodules (ATA guidelines are available at www.thyroid.org).
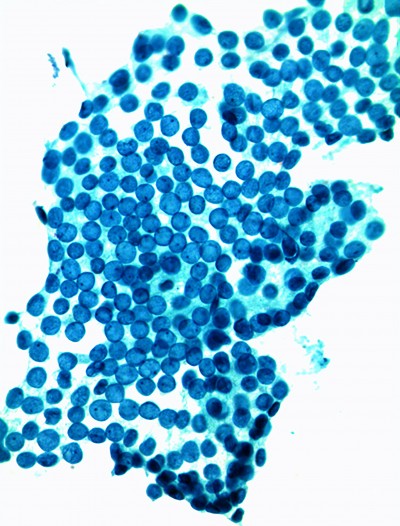
 Thyroid nodules become more common with increasing age. Random ultrasonographic studies have shown that 25-50% of adults have at least one thyroid nodule. However, the overall prevalence of malignant thyroid nodules is low. Fine needle aspiration (FNA) is the most accurate and cost-effective method for evaluating thyroid nodules. FNA with ultrasound guidance can be ordered to determine if thyroid nodules are malignant or benign. Cells from the thyroid withdrawn by FNA are sent to the pathology laboratory, where the cytology department screens for abnormalities.
Thyroid nodules become more common with increasing age. Random ultrasonographic studies have shown that 25-50% of adults have at least one thyroid nodule. However, the overall prevalence of malignant thyroid nodules is low. Fine needle aspiration (FNA) is the most accurate and cost-effective method for evaluating thyroid nodules. FNA with ultrasound guidance can be ordered to determine if thyroid nodules are malignant or benign. Cells from the thyroid withdrawn by FNA are sent to the pathology laboratory, where the cytology department screens for abnormalities.
The Bethesda System for Reporting Thyroid Cytopathology (BSRTC) recommends that all thyroid FNA reports include a “general diagnostic category” in the first diagnostic line (Benign, Indeterminate, Atypical, Suspicious, Malignant) followed by a description of cytologic findings. When indeterminate results are reported, there are additional options available for clinicians and their patients to obtain additional diagnostic information, which may help in deciding whether or not to have surgery.
Genetic mutations/translocations occur in 70-80% of thyroid malignancies. Newly developed molecular thyroid tests that identify genetic abnormalities associated with thyroid cancer have offered promise by adding helpful information to thyroid FNAs. For example, one test available identifies 17 molecular markers (mutations and translocations) of thyroid nodules that have been classified as indeterminate or suspicious by cytology. Another molecular test looks for gene mutations that have been shown to be associated with differentiated thyroid cancers in 70% of cases with positive results.
The majority of thyroid nodules are benign; however, 15-30% of thyroid nodules are classified as indeterminate or suspicious for malignancy. An indeterminate result can be frustrating to the pathologist, clinician and patient. Use of thyroid molecular testing can gain valuable information that may help more accurately classify indeterminate thyroid nodule results and can aid in surgical diagnostic decisions. Approximately 75,000 operations are performed each year in the U.S. for cytologically indeterminate nodules. This number may be reduced by one-third if results from molecular testing become more widely employed.
A recent New England Journal of Medicine article titled “Preoperative Diagnosis of Benign Thyroid Nodules with Indeterminate Cytology,” presents data supporting a more conservative approach for patients with cytologically indeterminate thyroid nodules on fine needle aspiration and the use of a new molecular test that provides additional data that can be used in decision making and management of indeterminate nodules.
References:
1 Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009;19:1167-214.
2 Cibas ES, Syed AZ. The Bethesda System for reporting thyroid cytopathology. Am J Clin Pathol 2009;132:658-65.